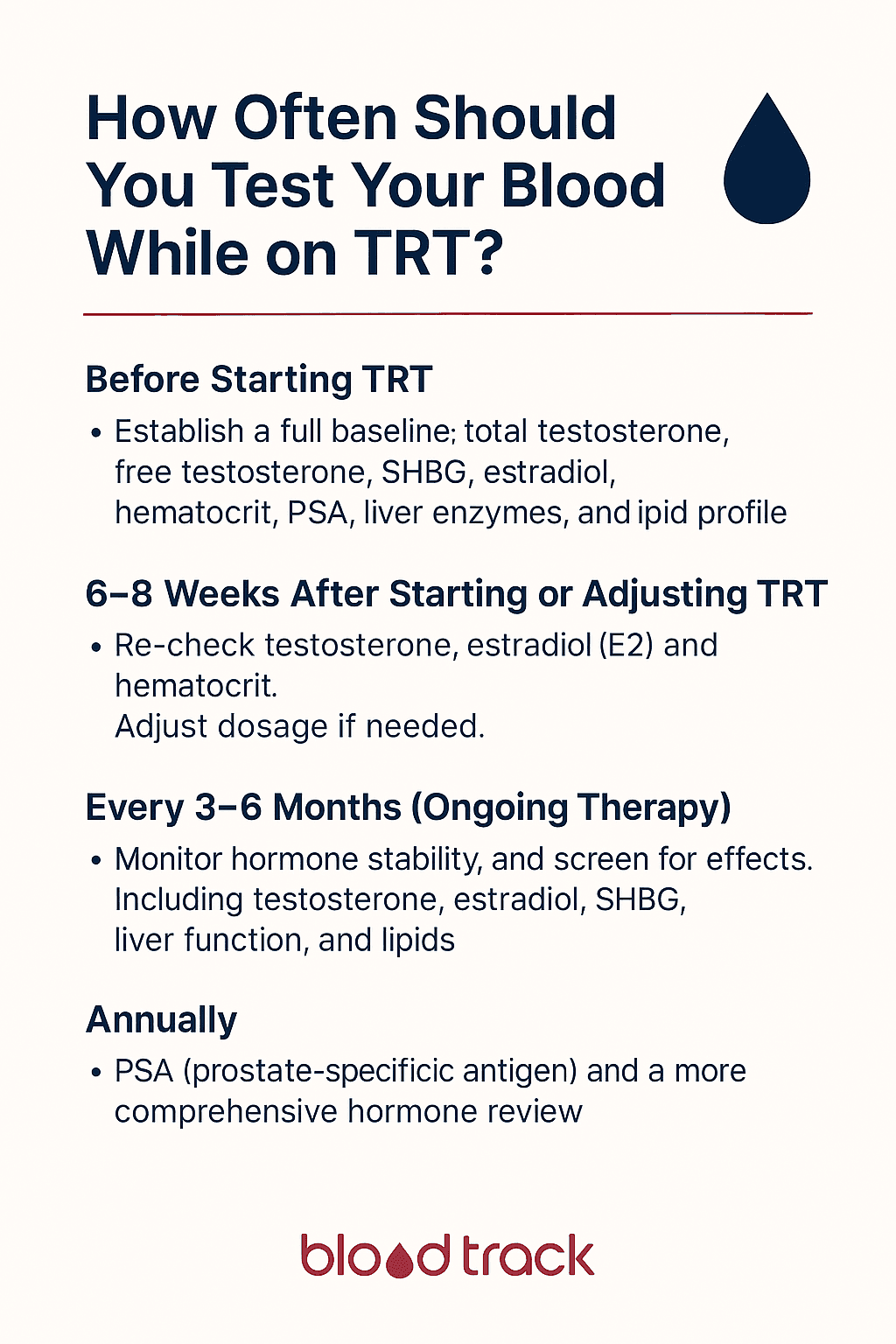
How Often Should You Test Your Blood While on TRT?
One of the most common questions from men starting testosterone replacement therapy is how frequently they need blood tests. The answer is not one-size-fits-all — it depends on where you are in your TRT journey, whether your protocol is stable, and what your individual risk factors are.
What is consistent across all clinical guidelines is this: regular blood testing on TRT is not optional. It is the only way to ensure your therapy is effective, safe, and properly dialled in. Skipping or delaying bloodwork is the single most common reason TRT protocols fail to deliver optimal results.
Blood Testing Timeline for TRT
Phase 1: Pre-TRT Baseline
Before starting testosterone therapy, you need a comprehensive baseline panel. This serves two critical purposes: confirming that you actually have low testosterone (hypogonadism) and establishing reference values for all markers that TRT can affect.
Baseline panel should include:
- Total testosterone — measured in the morning (before 10am) when levels peak
- Free testosterone — the biologically active fraction
- LH and FSH — to differentiate primary from secondary hypogonadism
- Estradiol (E2) — pre-treatment baseline
- SHBG — affects testosterone bioavailability
- Prolactin — rule out prolactinoma as a cause of low T
- Full blood count (FBC) — baseline haemoglobin and hematocrit
- Lipid panel — total cholesterol, LDL, HDL, triglycerides
- Liver function tests (LFTs) — ALT, AST, GGT
- Kidney function — eGFR, creatinine
- Fasting glucose and HbA1c — metabolic baseline
- PSA — prostate-specific antigen baseline for men over 40
- Thyroid function (TSH) — rule out thyroid dysfunction
- Vitamin D, iron studies — common co-deficiencies
Many clinicians recommend two separate morning testosterone measurements taken on different days before confirming a diagnosis of hypogonadism. A single low reading can be caused by acute illness, poor sleep, stress, or other transient factors.
Phase 2: Initial Monitoring (First 6 Months)
The first six months of TRT are the most critical period for blood testing. Your body is adapting to exogenous testosterone, and this is when most side effects emerge and dose adjustments are most frequently needed.
Recommended testing schedule:
- 6-8 weeks after starting TRT — first follow-up panel
- 3 months — second follow-up, especially if dose was adjusted
- 6 months — comprehensive panel to assess stability
What to test at each follow-up:
- Total and free testosterone (at trough — before your next injection)
- Estradiol (E2)
- Hematocrit and haemoglobin
- Liver enzymes (ALT, AST)
- Lipid panel
If any marker is outside the desired range, your clinician will adjust your dose and you should retest 6-8 weeks after the change. Do not adjust your dose and retest after only 2-3 weeks — testosterone levels take at least 4-6 weeks to reach a new steady state on injectable preparations.
Phase 3: Stable Maintenance (6+ Months)
Once your protocol is stable — meaning your testosterone is in the desired range, estradiol is balanced, hematocrit is safe, and you feel well — testing frequency can decrease.
Recommended maintenance schedule:
- Every 3-6 months: Core panel — testosterone (total and free), estradiol, hematocrit, FBC
- Every 6-12 months: Comprehensive panel adding lipids, liver function, fasting glucose, and HbA1c
- Annually: PSA (men over 40), full metabolic review, vitamin D, iron studies
If you make any changes to your protocol — dose adjustment, change in injection frequency, switching preparations, adding or removing an aromatase inhibitor — return to the Phase 2 schedule (retest at 6-8 weeks).
What Happens When You Skip Blood Tests
Many men feel great on TRT and assume blood tests are unnecessary if symptoms have improved. This is a dangerous assumption. Several TRT-related risks are clinically silent — meaning they cause no symptoms until they become serious:
- Elevated hematocrit — thickened blood increases stroke and clot risk with no symptoms until a cardiovascular event occurs. TRT-induced polycythemia is the most common haematological side effect.
- Dyslipidemia — TRT can suppress HDL cholesterol, increasing cardiovascular risk without any noticeable symptoms
- Liver enzyme elevation — particularly relevant for oral testosterone preparations or when combining TRT with other medications
- PSA elevation — while TRT does not cause prostate cancer, it can stimulate growth of existing prostate tissue. Rising PSA warrants further investigation.
Practical Tips for Consistent Testing
To get the most reliable and comparable results from your TRT blood tests:
- Always test at trough — draw blood immediately before your next injection to measure your lowest point
- Test in the morning — ideally before 10am, fasted for 8-12 hours
- Use the same lab — reference ranges and assays vary between laboratories. Consistency makes trends more reliable.
- Avoid intense exercise 24-48 hours before — heavy training can elevate liver enzymes, CK, and inflammatory markers
- Stay hydrated — dehydration artificially concentrates hematocrit and other markers
- Log your dose and timing — record your current dose, injection frequency, and time of last injection alongside each blood test
Cost and Access in Australia
In Australia, most TRT monitoring blood tests are covered by Medicare when ordered by your GP or specialist. Approximately 85% of pathology services are bulk-billed, meaning no out-of-pocket cost. If you are using a private TRT clinic, check whether they include blood testing in their fees or if you need to arrange testing independently through a Medicare-billing pathology provider.
For men on TRT through a GP, a standard monitoring panel (testosterone, FBC, lipids, liver function) can typically be ordered as a single pathology request and completed in one blood draw.
Tracking Your Results Over Time
Getting tested on schedule is the first step. The second — and equally important — step is tracking your results over time so you can see trends rather than isolated snapshots. BloodTrack lets you upload every blood test, visualise your testosterone, estradiol, hematocrit, and all other markers on trend charts, and share your complete history with your clinician at each appointment.
When your doctor can see your full TRT journey laid out visually — dose changes, marker responses, and symptom correlations — protocol decisions become faster, more confident, and more effective.
This article is for informational purposes only and does not constitute medical advice. Always consult your GP or endocrinologist for personalised guidance on TRT monitoring.